Monday, August 4, 2014
Goodbye Post!
I had a lot of fun writing these blog posts this semester. I really enjoyed researching topics to write up, and I feel like it was a good way to keep informed on what's going on the infectious diseases world. I also found out which topics I found interesting and which ones I did not. I was not surprised to learn that lab ops and policy was more interesting to me than current events. However, I did find that case studies were a lot more interesting than I had anticipated. My favorite post was about a new method for detecting antimicrobial resistance. I will probably not keep up with this blog, but I will probably archive it and leave it up for the world. I hope you all have a great fall semester!
Sunday, August 3, 2014
Containing Ebola Virus
One of the most important issues hospitals and other healthcare providers face when treating highly infectious patients is keeping other patients in the facility safe. Highly infectious patients easily transmit disease to other people, and PPE (personal protective equipment) may not be enough to protect patients if a particular infection is spread through respiratory droplets or otherwise able to spread through the air. This concern is coming to the forefront now that an Ebola victim is being transported to Emory University Hospital for treatment after they were infected caring for other victims in the African outbreak.
 The CDC recommendations which came out Friday afternoon recommend hospital workers in charge of Ebola patients should wear gloves, a fluid-resistant gown, eye protection, and a face mask. Double sets of gloves, shoe covers, or leg covers are recommended if there is a large amount of blood or bodily fluid present. The PPE is then removed when the healthcare worker exits the room, placed into specially marked waste bags, and burned. Emory University Hospital has a special wing that is separate from the rest of the hospital that was created to treat patients of pandemics or bioterrorism attacks. Additionally, the Ebola patient will likely be quarantined in a negative-pressure room with isolated air flow, even though Ebola is not spread through the air.
The CDC recommendations which came out Friday afternoon recommend hospital workers in charge of Ebola patients should wear gloves, a fluid-resistant gown, eye protection, and a face mask. Double sets of gloves, shoe covers, or leg covers are recommended if there is a large amount of blood or bodily fluid present. The PPE is then removed when the healthcare worker exits the room, placed into specially marked waste bags, and burned. Emory University Hospital has a special wing that is separate from the rest of the hospital that was created to treat patients of pandemics or bioterrorism attacks. Additionally, the Ebola patient will likely be quarantined in a negative-pressure room with isolated air flow, even though Ebola is not spread through the air.
Dr. William Schaffner, infectious disease specialist and preventative medicine professor at Vanderbilt University, reminds us that "the system for keeping bad germs under control is simple...The trick will be to do it rigorously at all times." An important lesson was learned in 2003 during the SARS outbreak: hospital workers will shortcut PPE because they were busy, "or because familiarity breeds if not contempt then casualness". Hopefully, history will not repeat itself once the Ebola patient arrives at Emory.
Sources
Article: http://www.npr.org/blogs/health/2014/08/01/337140082/how-u-s-hospitals-contain-deadly-germs-like-ebola-virus
Picture: http://app1.unmc.edu/nursing/heroes/images/heroesDoffingYourHospitalPPE-Poster2012.jpg
 The CDC recommendations which came out Friday afternoon recommend hospital workers in charge of Ebola patients should wear gloves, a fluid-resistant gown, eye protection, and a face mask. Double sets of gloves, shoe covers, or leg covers are recommended if there is a large amount of blood or bodily fluid present. The PPE is then removed when the healthcare worker exits the room, placed into specially marked waste bags, and burned. Emory University Hospital has a special wing that is separate from the rest of the hospital that was created to treat patients of pandemics or bioterrorism attacks. Additionally, the Ebola patient will likely be quarantined in a negative-pressure room with isolated air flow, even though Ebola is not spread through the air.
The CDC recommendations which came out Friday afternoon recommend hospital workers in charge of Ebola patients should wear gloves, a fluid-resistant gown, eye protection, and a face mask. Double sets of gloves, shoe covers, or leg covers are recommended if there is a large amount of blood or bodily fluid present. The PPE is then removed when the healthcare worker exits the room, placed into specially marked waste bags, and burned. Emory University Hospital has a special wing that is separate from the rest of the hospital that was created to treat patients of pandemics or bioterrorism attacks. Additionally, the Ebola patient will likely be quarantined in a negative-pressure room with isolated air flow, even though Ebola is not spread through the air.Dr. William Schaffner, infectious disease specialist and preventative medicine professor at Vanderbilt University, reminds us that "the system for keeping bad germs under control is simple...The trick will be to do it rigorously at all times." An important lesson was learned in 2003 during the SARS outbreak: hospital workers will shortcut PPE because they were busy, "or because familiarity breeds if not contempt then casualness". Hopefully, history will not repeat itself once the Ebola patient arrives at Emory.
Sources
Article: http://www.npr.org/blogs/health/2014/08/01/337140082/how-u-s-hospitals-contain-deadly-germs-like-ebola-virus
Picture: http://app1.unmc.edu/nursing/heroes/images/heroesDoffingYourHospitalPPE-Poster2012.jpg
Saturday, July 26, 2014
Parasite Infection as a Treatment for Crohn's Disease
A new paper suggests that patients with intestinal disorders, such as Crohn's disease or inflammatory bowel disease (IBS), would gain from infection with intestinal parasites.Julius Lukes, one of the co-authors of the paper, and other scientists in the Canadian Institute for Advanced Research (CIFAR) Integrated Microbial Biodiversity program have begun to focus on eukaryotes which live within the human body in recent years - what they are calling the "eukaryome". Lukes asserts that most parasites are not harmful to otherwise healthy patients with low parasite loads. To prove his point, he ingested several eggs of Diphyllobothrium latum (picture below), a tapeworm commonly acquired by eating under-cooked fish. After a year, the parasites are estimated to be 12 feet in length, and Julius reports he is feeling fine.
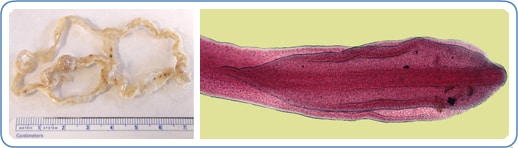
The theory behind the deliberate infection of these patients with parasites is an extension of the "Old Friends Hypothesis", which is based on the idea that they evolved with us and have been inside humans for most of our history. These parasites, which include hookworms, tapeworms, and Blastocystis species, are thought to "distract" the immune system and prevent it from overreacting to normal stress and reducing inflammation in the intestines. These parasites are commonly thought to cause vitamin deficiency, anemia, and diarrhea, but Lukes says that a critical review of the evidence shows "no negative impact in well-nourished people with low overall parasite loads". The hypothesis is still in the early stages of testing, but similar strategies have worked for viral infections.
Sources
Article: http://www.medicalnewstoday.com/releases/280085.php
Picture: http://www.cdc.gov/parasites/images/diphyllobothrium/home_page_image_diphyllobothrium.jpg
Saturday, July 19, 2014
Cryptococcus gattii in the Pacific Northwest
Cryptococcus gattii is a tropical fungus which causes severe neurological disease in those it infects. In 1999, C. gattii was isolated on Vancouver Island, British Columbia, Canada. In Canada, the fungus evolved into a virulent pulmonary form which has caused dozens of deaths. Since 1999, C. gattii has spread to mainland Canada, Washington state, and Oregon. In Oregon, a new strain of C. gattii was discovered which has increased lethality. This strain has spread through the Pacific Northwest.
These new strains of C. gattii have been investigated by a team from the Translational Genomics Research Institute (TGen), led by David Engelthaler, Director of Programs and Operations. This team contained 24 researched from 13 institutions in 7 nations. They sequenced 115C. gattii genomes from 15 countries. Their results, published in the journal mBio, identify "several genes that may make the outbreak strains more capable of surviving colder environments and that make it more harmful in the lungs". These genes are also possible targets for new diagnostic tests, therapeutic drugs, or preventative vaccines. This study also "provide[s] evidence that the Pacific Northwest strains originated from South America", most likely originating from Brazil.
The study, "Cryptococcus gattii in North American Pacific Northwest: whole population genome analysis provides insights into species evolution and dispersal", warns that the virus is easily adaptable to new environments and warrants public heath vigilance, even in areas where C. gattii is not thought to be endemic.

Source: http://www.medicalnewstoday.com/releases/279696.php
Image: http://www.cdc.gov/fungal/images/cryptococcus-gattii-lifecycle.jpg
These new strains of C. gattii have been investigated by a team from the Translational Genomics Research Institute (TGen), led by David Engelthaler, Director of Programs and Operations. This team contained 24 researched from 13 institutions in 7 nations. They sequenced 115C. gattii genomes from 15 countries. Their results, published in the journal mBio, identify "several genes that may make the outbreak strains more capable of surviving colder environments and that make it more harmful in the lungs". These genes are also possible targets for new diagnostic tests, therapeutic drugs, or preventative vaccines. This study also "provide[s] evidence that the Pacific Northwest strains originated from South America", most likely originating from Brazil.
The study, "Cryptococcus gattii in North American Pacific Northwest: whole population genome analysis provides insights into species evolution and dispersal", warns that the virus is easily adaptable to new environments and warrants public heath vigilance, even in areas where C. gattii is not thought to be endemic.
Source: http://www.medicalnewstoday.com/releases/279696.php
Image: http://www.cdc.gov/fungal/images/cryptococcus-gattii-lifecycle.jpg
Sunday, July 13, 2014
A New Rapid Test for Detecting Multi-Drug Resistance
One of the major complications of treating bacterial infections is the potential for multi-drug resistant (MDR), extensively drug-resistant (XDR), or pan-drug-resistant (PDR) organisms. Multi-drug resistance is defined as "non-susceptibility to at least one agent in three or more antimicrobial categories", XDR is defined as "non-susceptibility to at least one agent in two or fewer categories", and PDR is defined as non-susceptibility to all agents in all antimicrobial categories" (1). Fortunately, XDR and PDR organisms are much fewer in number than MDR organisms. However, antimicrobial resistance has increased dramatically over the past 20 years, particularly in regards to gram-negative rods, and broad-spectrum antibiotics such as cephalosporins and carbapenems (which used to be last-resort options) are now losing their efficacy.

A new rapid test, CarbAcineto NP, has been developed by Patrice Nordmann and Laurent Poirel which detects the presence of carbapenemase in Acinetobacter baumanii. This test detects "the acidification properties generated by the enzymatic hydrolysis of a carbapenem, imipenem, when it is cleaved by a carbapenemase". The acid produced by the breakdown of imipenem causes a pH indicator to turn from red to yellow. Either isolated bacteria or swabs of a site infection can be used in the test, which produces results in less than 2 hours, much faster than the 24-72 hours required for current methods. This new rapid test allows treatment decisions to be made much more quickly and effectively, as well as allowing for the identification of potential MDR organisms as a screening tool.
Article Sources
(1): http://www.ncbi.nlm.nih.gov/pubmed/21793988
Article: http://www.sciencedaily.com/releases/2014/06/140626095705.htm
Image: http://bacteriasactuaciencia.blogspot.com/2013/10/esperanza-en-la-lucha-contra.html
A new rapid test, CarbAcineto NP, has been developed by Patrice Nordmann and Laurent Poirel which detects the presence of carbapenemase in Acinetobacter baumanii. This test detects "the acidification properties generated by the enzymatic hydrolysis of a carbapenem, imipenem, when it is cleaved by a carbapenemase". The acid produced by the breakdown of imipenem causes a pH indicator to turn from red to yellow. Either isolated bacteria or swabs of a site infection can be used in the test, which produces results in less than 2 hours, much faster than the 24-72 hours required for current methods. This new rapid test allows treatment decisions to be made much more quickly and effectively, as well as allowing for the identification of potential MDR organisms as a screening tool.
Article Sources
(1): http://www.ncbi.nlm.nih.gov/pubmed/21793988
Article: http://www.sciencedaily.com/releases/2014/06/140626095705.htm
Image: http://bacteriasactuaciencia.blogspot.com/2013/10/esperanza-en-la-lucha-contra.html
Saturday, July 5, 2014
Biofilms and Catheters
Biofilms are formed by many bacteria, some that are harmful and some that are not. These films are slimy coatings that protect bacteria against antibiotics, our immune systems, cleaning agents, and other environmental dangers. In hospitals, biofilms that form inside catheters or around implanted medical devices can lead to infections, especially from Staphylococcus aureus.
Researchers at Princeton University were able to observe how biofilms form within small tubes such as catheters. Typically, biofilms build up into thick layers on surfaces. In flowing liquids, biofilms for string-like filaments that float within the fluid. The researchers were first able to observe filament formation in a solution of Pseudomonas aeruginosa. Filaments formed by P. aeruginosa took around 50 hours to clog the tubing. When researchers repeated the experiment with S. aureus, the tubes clogged within a few hours. They then coated the tubes with plasma to imitate how the organism would act within an intravenous catheter. These tubes were clogged in a few minutes.
Howard Stone, a Princeton researcher, says he is unsure how the organism is able to form these filaments so quickly, but the knowledge will assist with designing medicals tools and devices that are more resistant to colonization. Stone also pointed out that the concentrations of bacteria used in the experiments was much higher than those typically found inside medical devices. Breaking up the biofilms and preventing them from forming could be the next step in treatment of these organisms.
Source: http://www.npr.org/blogs/health/2014/06/27/325502998/sticky-streamers-of-staph-bacteria-may-clog-up-medical-devices
Sunday, June 29, 2014
MERS
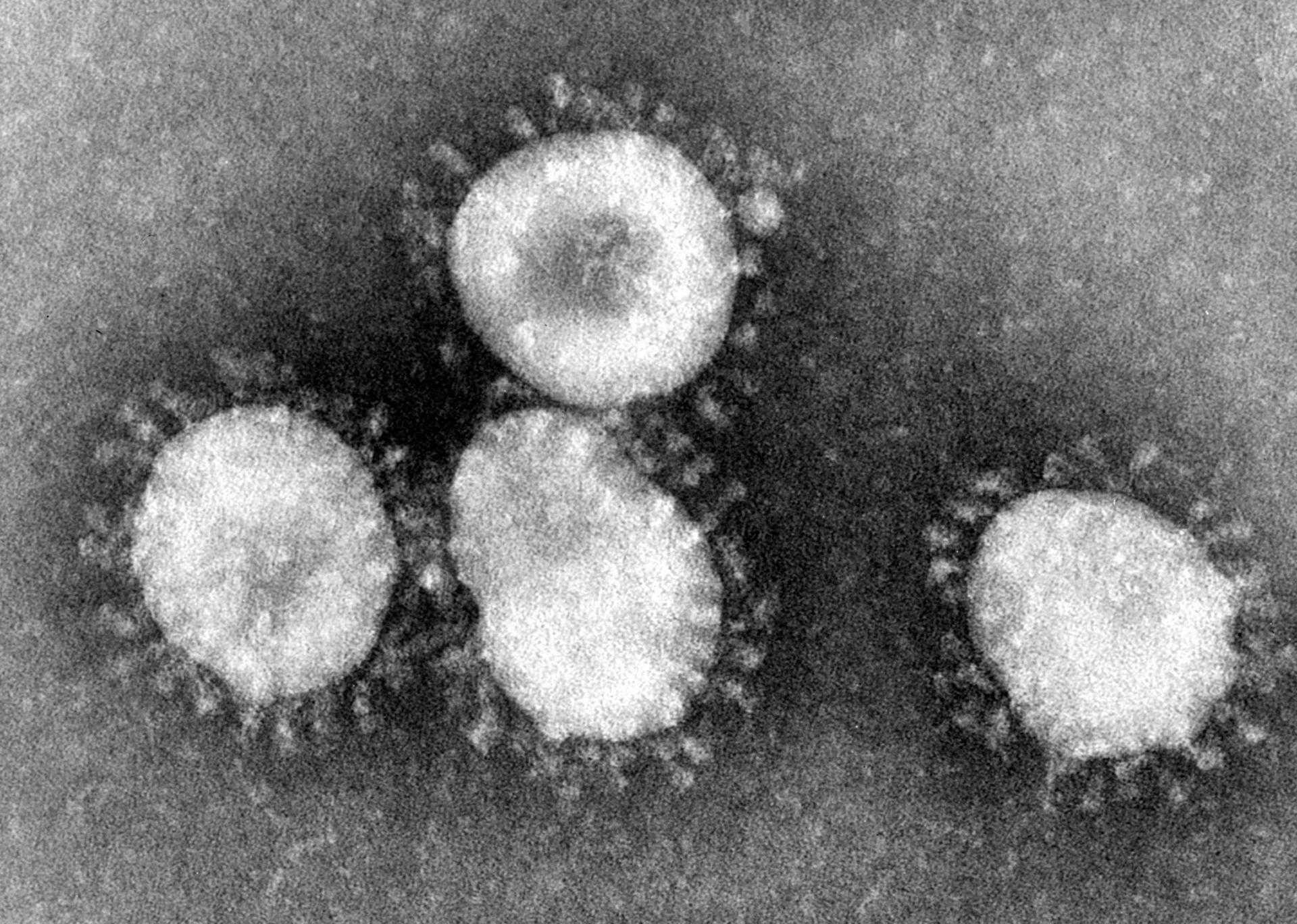
MERS, or Middle Eastern Respiratory Syndrome, is a viral illness which appeared in Saudi Arabia in 2012. MERS is a coronavirus, similar in structure to rhinoviruses which cause the common cold and SARS. The first symptoms of MERS are fever, cough, and shortness of breath. Since 2012, MERS has spread across the Middle East, and has been found in camels in Qatar, Oman, and Egypt in addition to Saudi Arabia. The exact source of the infection is unknown, but camels are a strong suspect. MERS cases outside the Middle East are associated with travel, and are not endemic. According to the World Health Organization (WHO), there have been 820 cases of MERS and 286 deaths. Saudi Arabia has reported 113 cases and 34 deaths. Currently, there is no vaccine available for MERS.
Reports of MERS cases began to increase in March of this year, but has begun to decrease again. However, some scientists at WHO are concerned that the annual pilgrimage (Hajj) to Saudi Arabia in October will further increase its spread. Currently, MERS does not easily spread from person-to-person (most cases are spread camel-to-person), but the increased number of people exposed to camels in the coming months could allow the virus to mutate. Saudi Arabian health officials say they have increased surveillance and infection control measures in anticipation of the Hajj.
Resources
http://www.nbcnews.com/storyline/mers-mystery/mers-outbreak-could-spread-annual-pilgrimage-officials-n132866
http://www.cdc.gov/coronavirus/mers/faq.html
http://www.bbc.com/news/health-28044151
Reports of MERS cases began to increase in March of this year, but has begun to decrease again. However, some scientists at WHO are concerned that the annual pilgrimage (Hajj) to Saudi Arabia in October will further increase its spread. Currently, MERS does not easily spread from person-to-person (most cases are spread camel-to-person), but the increased number of people exposed to camels in the coming months could allow the virus to mutate. Saudi Arabian health officials say they have increased surveillance and infection control measures in anticipation of the Hajj.
Resources
http://www.nbcnews.com/storyline/mers-mystery/mers-outbreak-could-spread-annual-pilgrimage-officials-n132866
http://www.cdc.gov/coronavirus/mers/faq.html
http://www.bbc.com/news/health-28044151
Sunday, June 22, 2014
Making Blood Culture Workups More Efficient
A major problem with blood culture workups is that it is often difficult to determine a true positive (pathogen) result from a false positive (contaminant) result. One solution is to adjust the testing algorithm in place. In 1970, it was shown that 11% of contaminated cultures had additional positive cultures, while 69% of clinically significant cultures had multiple positive cultures. In the proposed algorithm (summarized right), any
 isolates that are typically contaminants that are not present in follow-up cultures are reported as contaminants. To confirm the accuracy of the new algorithm, a nurse epidemiologist and an infectious diseases physician reviewed the patient charts.
isolates that are typically contaminants that are not present in follow-up cultures are reported as contaminants. To confirm the accuracy of the new algorithm, a nurse epidemiologist and an infectious diseases physician reviewed the patient charts.
Overall, organisms considered to be contaminants (CNS, diphthroids, Micrococcus spp, Bacillus spp, and viridans streptococci) were identified in 495/1040 positive blood cultures. Of the 495, 286 were classified as contaminants due to negative follow-up cultures, 171 were investigated by a pathology resident, and 15 were classified as pathogens (viridans strep with positive follow-up cultures). The majority (62%) of the contaminants were identified as CNS.
Two types of errors, VM (very major) and M (major) were used to determine the success of the new algorithm. A "very major error" occurred if an isolate that was classified as a contaminant was determined to be clinically significant after chart review. A "major" error occurred if an isolate was classified as indeterminate or pathogenic and was later determined to be not clinically significant. VM errors occurred in 6.3% of cases and M errors occurred in 6.6% of cases. Further adjustment of this algorithm may decrease the error rate in the future, but the algorithm was determined "acceptable" by the authors of this study.
Source: http://jcm.asm.org/content/40/7/2437.full
isolates that are typically contaminants that are not present in follow-up cultures are reported as contaminants. To confirm the accuracy of the new algorithm, a nurse epidemiologist and an infectious diseases physician reviewed the patient charts.Overall, organisms considered to be contaminants (CNS, diphthroids, Micrococcus spp, Bacillus spp, and viridans streptococci) were identified in 495/1040 positive blood cultures. Of the 495, 286 were classified as contaminants due to negative follow-up cultures, 171 were investigated by a pathology resident, and 15 were classified as pathogens (viridans strep with positive follow-up cultures). The majority (62%) of the contaminants were identified as CNS.
Two types of errors, VM (very major) and M (major) were used to determine the success of the new algorithm. A "very major error" occurred if an isolate that was classified as a contaminant was determined to be clinically significant after chart review. A "major" error occurred if an isolate was classified as indeterminate or pathogenic and was later determined to be not clinically significant. VM errors occurred in 6.3% of cases and M errors occurred in 6.6% of cases. Further adjustment of this algorithm may decrease the error rate in the future, but the algorithm was determined "acceptable" by the authors of this study.
Source: http://jcm.asm.org/content/40/7/2437.full
Friday, June 13, 2014
PED Virus Increasing Pork Prices
In May 2013, porcine epidemic diarrhea virus (PEDv) was isolated in hog herds in the United States. PEDv cause diarrhea and vomiting in pigs (morbidity near 100%) with variable mortality. Older pigs are more likely to survive the virus than young pigs (mortality 50-100%). The virus has an incubation period of 3-4 days, and is spread more slowly than other types of swine gastroenteritis. Pigs who recover do so within 7-10 days of symptom onset. The virus is spread through a fecal-oral route, but fomites and contaminated equipment may spread the virus as well.

PEDv was first reported in the United Kingdom in 1971, and has spread to several countries since then.
PEDv is a Coronavirus, containing an enveloped ssRNA genome. The virus does not appear to have jumped to humans in the 40 years since its discovery.
Global AgriTrends speculates that up to 4.5% of pigs, or 4.5 million hogs, in the US may be killed by PEDv this year. Some farms have lost 10% of their herds already. Pork prices are expected to increase 3% this year, compared to 0.9% last year. A vaccine is not yet available for the virus in the US, but there are vaccines currently available in South Korea, Japan, and China.
PEDv was first reported in the United Kingdom in 1971, and has spread to several countries since then.
PEDv is a Coronavirus, containing an enveloped ssRNA genome. The virus does not appear to have jumped to humans in the 40 years since its discovery.
Global AgriTrends speculates that up to 4.5% of pigs, or 4.5 million hogs, in the US may be killed by PEDv this year. Some farms have lost 10% of their herds already. Pork prices are expected to increase 3% this year, compared to 0.9% last year. A vaccine is not yet available for the virus in the US, but there are vaccines currently available in South Korea, Japan, and China.
Sunday, June 8, 2014
Bacteria Cultured from a Bear Bite
One of the dangers of an animal bite (aside from the trauma of the bite itself) is the possibility of infection due to flora in the mouth of the animal. If an infection does develop from an animal bite, knowing the flora present is helpful in choosing antibiotics that will be effective. Most animals that interact with humans (cats, dogs, etc) have well-defined flora. Less is known about other animals, such as bears, that rarely bite humans.
A case report from 2004 describes the bacteria cultured from a bite wound inflicted on a hunter by a grizzly bear in Canada. Cultures taken about 12 hours after the bite grew Serratia fonticola, Serratia
 marcescens (used to draw a raptor, right), Aeromonas hydrophila, Bacillus cereus, and Enterococcus durans. No anaerobes were isolated from the wound. The patient was given 1 week of piperacillin-tazobactam therapy followed by amoxicillin-clavulanate and ciprofloxacin for 3 weeks as prophylactic treatment.
marcescens (used to draw a raptor, right), Aeromonas hydrophila, Bacillus cereus, and Enterococcus durans. No anaerobes were isolated from the wound. The patient was given 1 week of piperacillin-tazobactam therapy followed by amoxicillin-clavulanate and ciprofloxacin for 3 weeks as prophylactic treatment.
Infection after a bear bite is common, with around 44% of patients showing infection. However, few of these bite wounds have been cultured for identification of flora, so there is limited knowledge of what is common or what antimicrobials are appropriate for treatment. Some scientists hypothesize that oral flora of bears will be similar to that of dogs, as well as being highly variable depending on the foraging environment and habits of a particular bear.
More information about the patient and his clinical outcomes can be found here: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC446265/#__ffn_sectitle
A case report from 2004 describes the bacteria cultured from a bite wound inflicted on a hunter by a grizzly bear in Canada. Cultures taken about 12 hours after the bite grew Serratia fonticola, Serratia

Infection after a bear bite is common, with around 44% of patients showing infection. However, few of these bite wounds have been cultured for identification of flora, so there is limited knowledge of what is common or what antimicrobials are appropriate for treatment. Some scientists hypothesize that oral flora of bears will be similar to that of dogs, as well as being highly variable depending on the foraging environment and habits of a particular bear.
More information about the patient and his clinical outcomes can be found here: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC446265/#__ffn_sectitle
Saturday, May 31, 2014
Malaria Vaccine in the Works
Malaria is a disease caused by parasitic organisms of the Plasmodium family that are transmitted by the bites of infected Anopheles mosquitoes. Of the four species that cause illness in humans, P. falciparum is the most common and the most deadly. Malaria is most common in Africa, but is present throughout the world. Malaria is an acute febrile illness, with symptoms such as fever, nausea, or vomiting appearing 10-15 days after infection. If treatment is not begun within 24 hours, P. falciparum malaria can cause severe illness or even death.
 A new vaccine for malaria is currently in early stage trials with promising results! The vaccine was developed after a survey of Tanzanian children found that 6% of them had antibodies to a protein crucial to the parasite's development. The antibody prevents the parasite, Plasmodium falciparum (picture right: organisms in intracellular phase), from reproducing within the blood cell. This allows the spleen and macrophages time to remove the damaged cells from circulation. The children with the antibody did not suffer from severe malaria, consistent with a previous study in Kenyan adolescents. This new vaccine is one of around 100 vaccines that have been developed since 1980, but is the first to focus on the parasite once it has entered the body.
A new vaccine for malaria is currently in early stage trials with promising results! The vaccine was developed after a survey of Tanzanian children found that 6% of them had antibodies to a protein crucial to the parasite's development. The antibody prevents the parasite, Plasmodium falciparum (picture right: organisms in intracellular phase), from reproducing within the blood cell. This allows the spleen and macrophages time to remove the damaged cells from circulation. The children with the antibody did not suffer from severe malaria, consistent with a previous study in Kenyan adolescents. This new vaccine is one of around 100 vaccines that have been developed since 1980, but is the first to focus on the parasite once it has entered the body.
Picture: http://lib.jiangnan.edu.cn/ASM/257-1.jpg
References
http://www.forbes.com/sites/paulrodgers/2014/05/23/has-malaria-met-its-match/
http://www.who.int/mediacentre/factsheets/fs094/en/
 A new vaccine for malaria is currently in early stage trials with promising results! The vaccine was developed after a survey of Tanzanian children found that 6% of them had antibodies to a protein crucial to the parasite's development. The antibody prevents the parasite, Plasmodium falciparum (picture right: organisms in intracellular phase), from reproducing within the blood cell. This allows the spleen and macrophages time to remove the damaged cells from circulation. The children with the antibody did not suffer from severe malaria, consistent with a previous study in Kenyan adolescents. This new vaccine is one of around 100 vaccines that have been developed since 1980, but is the first to focus on the parasite once it has entered the body.
A new vaccine for malaria is currently in early stage trials with promising results! The vaccine was developed after a survey of Tanzanian children found that 6% of them had antibodies to a protein crucial to the parasite's development. The antibody prevents the parasite, Plasmodium falciparum (picture right: organisms in intracellular phase), from reproducing within the blood cell. This allows the spleen and macrophages time to remove the damaged cells from circulation. The children with the antibody did not suffer from severe malaria, consistent with a previous study in Kenyan adolescents. This new vaccine is one of around 100 vaccines that have been developed since 1980, but is the first to focus on the parasite once it has entered the body.Picture: http://lib.jiangnan.edu.cn/ASM/257-1.jpg
References
http://www.forbes.com/sites/paulrodgers/2014/05/23/has-malaria-met-its-match/
http://www.who.int/mediacentre/factsheets/fs094/en/
Friday, May 23, 2014
Lemierre's Syndrome: A Case Report

Before the introduction of antibiotics, Lemierre's syndrome had a mortality rate around 90%. Currently, the mortality rate of correctly-diagnosed cases is around 5%. Fewer than 100 cases have been described since 1974, and the condition has a incidence rate of 3.6 cases per 1 million. This syndrome is characterized by a recent history of oropharyngitis with persistent fevers, followed by septic thrombophlebitis (swelling of a vein caused by a blood clot) of the internal jugular vein as well as dissemination of the infection to multiple sites. Lemierre's syndrome should be suspected in patients who present with pharyngitis and high-grade fevers (39-41C) plus thrombophlebitis or sepsis.

Case Report
A previously healthy 44 year old female presented with a 3 day history of worsening sore throat predominantly on the left side with fever, pain while swallowing, and vomiting. Upon examination, she was febrile, hypotensive, and tachycardic. Her left tonsil was displaced, and her lymph nodes were swollen and tender. Laboratory testing showed her WBC to be elevated with a decreased platelet count, as well as decreased liver and kidney function. A CT scan (right) showed a mass in the left peritonsillar region (arrow). Drainage of the mass was delayed due to the patient's unstable condition. The patient deteriorated rapidly, developing acute renal failure, encephalopathy, respiratory failure, and bilateral pleural effusions. She was placed on mechanical ventilation and dialysis. Blood cultures grew F. necrophorum and the patient's antibiotics were adjusted to piperacillin-tazobactam and metronidazole. The patient was extubated on her ninth day of admission, and discharged on the thirteenth.
References
SBA picture: http://pictures.life.ku.dk/atlas/microatlas/veterinary/bacteria/Fusobacterium_necrophorum_A/fusobacteriumnecrophoruma.jpg
Case Study: : Arora T, Wright D (2014) Lemierre’s Syndrome in an Adult: A Case Review. Otolaryngology 4: 167. doi:10.4172/2161-119X.1000167
Friday, May 16, 2014
Ebola!

Ebolavirus infection is fatal in 50-90% of cases, with some strains less virulent (50-60%) and others more virulent (80-90%). Symptoms appear 2-21 days post-exposure with a rapid onset. Initial symptoms are flu-like, but quickly progress to more serious symptoms such as chest pain, red eyes, skin rash, jaundice, hiccups, or bleeding. Laboratory findings of interest are low WBC/platelet counts with elevated liver enzymes. Definitive diagnosis of ebolavirus occurs through ELISA, antigen detection or serum neutralization tests, RT-PCR assays, electron microscopy, or viral culture.
The virus produces proteins that increase blood vessel permeability, causing hemorrhage. Ebolavirus may also prevent the body from mounting an appropriate immune response through an unknown mechanism. One theory is that the virus overwhelms the immune system using a cytokine storm, sending the patient into shock. Another theory is the virus prevents the immune system from mounting a response at all by reducing interferon activity within the cells (normally, this activity would signal NK cells or T cells that a cell has been taken over by a virus and mark it for destruction).
Unfortunately, there is no treatment for ebolavirus, but a vaccine is in clinical trials. Infected patients are placed into quarantine and receive supportive therapy, such as pain medicine or fluids. Death results from pulmonary or gastrointestinal hemorrhage, hepatitis, or encephalitis one to two weeks after the onset of symptoms. Patients who recover may remain infectious for several weeks after symptoms clear.
References
Picture: http://edwardmd.files.wordpress.com/2013/11/ebola1.jpg
1. Basler Christopher, et al. The Ebola Virus VP35 Protein Inhibits Activation of Interferon Regulatory Factor 3. Journal of Virology. July 2003: 88(11).
2. CDC. Ebola Hemorrhagic Fever. CDC Viral Hemorrhagic Fevers. 2014. Available at: http://www.cdc.gov/vhf/ebola/. Accessed May 16, 2014.
3. Federation of American Scientists. Ebola Fact Sheet. FAS Biosecurity Fact Sheets. Available at: http://www.fas.org/programs/ssp/bio/factsheets/ebolafactsheet.html. Accessed May 16, 2014.
4. Villinger Francois, et al. Markedly Elevated Levels of Interferon (IFN)-y, IFN-a, Interleukin (IL)-2, and Tumor Necrosis Factor-a Associated with Fatal Ebola Virus Infection. The Journal of Infectious Diseases. 1999: 179 pp S188-S191.
5. WHO. Ebola virus disease. WHO Media Centre Fact Sheets. 2014. Available at: http://www.who.int/mediacentre/factsheets/fs103/en/. Accessed May 16, 2014.
Tuesday, May 6, 2014
Welcome!
Hello blog readers and welcome to my blog, Microbi-blog-ogy.
I am a graduate student in UAB's CLS program, and my interests include bluegrass music, duathlon/triathlon, and crossword puzzles. My favorite color is purple, and my favorite movie is O Brother, Where Art Thou?. I received my Bachelor's degree in Laboratory Technology from Auburn University in 2013. My skills include LaTeX, time management, computer applications, and accepting visual, auditory, and tactile inputs and translating them into kinesthetic outputs
Currently, I am taking an infectious diseases course as part of my Master's degree program. This blog will showcase topics of interest that I encounter throughout this course.
I am a graduate student in UAB's CLS program, and my interests include bluegrass music, duathlon/triathlon, and crossword puzzles. My favorite color is purple, and my favorite movie is O Brother, Where Art Thou?. I received my Bachelor's degree in Laboratory Technology from Auburn University in 2013. My skills include LaTeX, time management, computer applications, and accepting visual, auditory, and tactile inputs and translating them into kinesthetic outputs
Currently, I am taking an infectious diseases course as part of my Master's degree program. This blog will showcase topics of interest that I encounter throughout this course.
Subscribe to:
Comments (Atom)