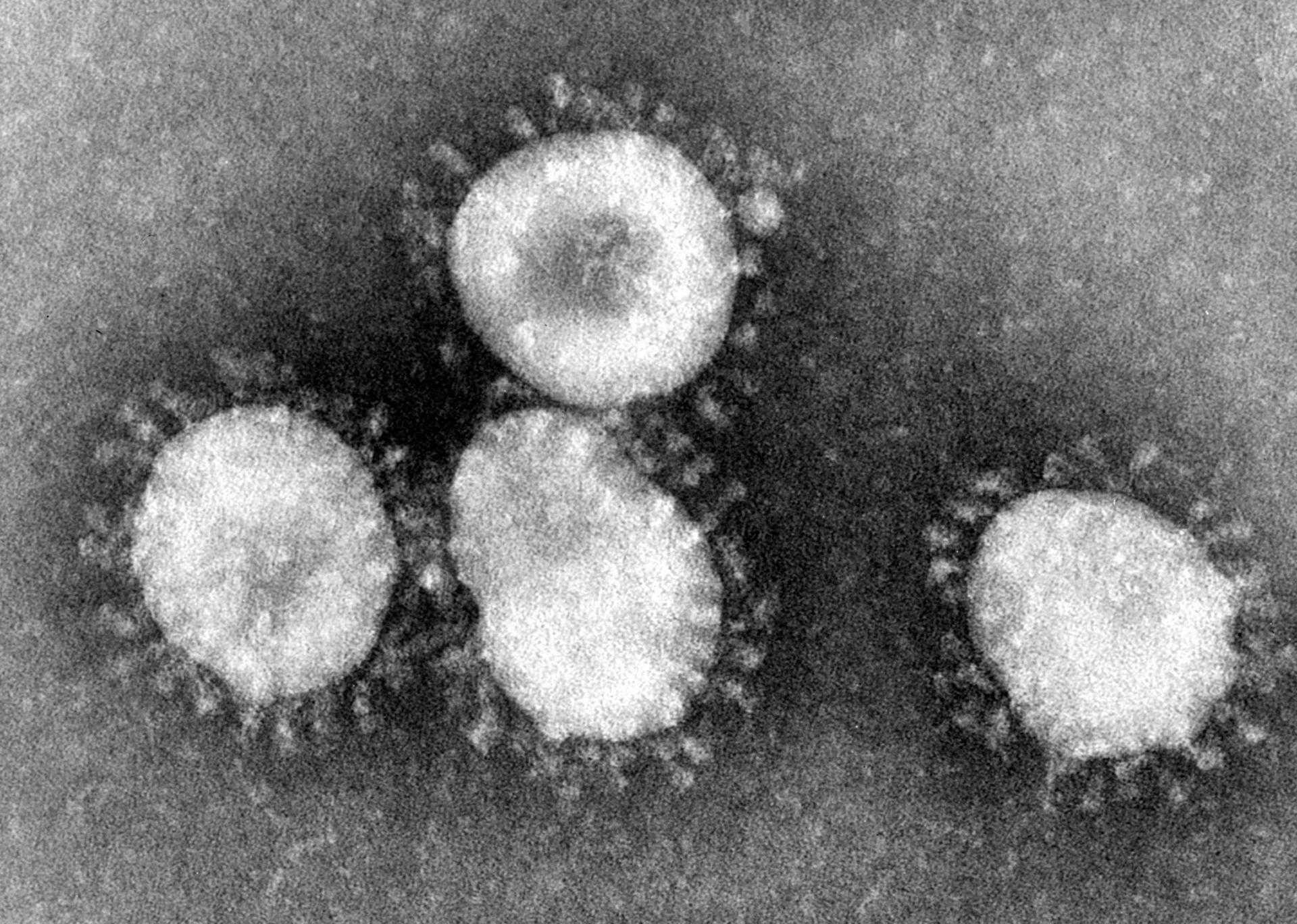
MERS, or Middle Eastern Respiratory Syndrome, is a viral illness which appeared in Saudi Arabia in 2012. MERS is a coronavirus, similar in structure to rhinoviruses which cause the common cold and SARS. The first symptoms of MERS are fever, cough, and shortness of breath. Since 2012, MERS has spread across the Middle East, and has been found in camels in Qatar, Oman, and Egypt in addition to Saudi Arabia. The exact source of the infection is unknown, but camels are a strong suspect. MERS cases outside the Middle East are associated with travel, and are not endemic. According to the World Health Organization (WHO), there have been 820 cases of MERS and 286 deaths. Saudi Arabia has reported 113 cases and 34 deaths. Currently, there is no vaccine available for MERS.
Reports of MERS cases began to increase in March of this year, but has begun to decrease again. However, some scientists at WHO are concerned that the annual pilgrimage (Hajj) to Saudi Arabia in October will further increase its spread. Currently, MERS does not easily spread from person-to-person (most cases are spread camel-to-person), but the increased number of people exposed to camels in the coming months could allow the virus to mutate. Saudi Arabian health officials say they have increased surveillance and infection control measures in anticipation of the Hajj.
Resources
http://www.nbcnews.com/storyline/mers-mystery/mers-outbreak-could-spread-annual-pilgrimage-officials-n132866
http://www.cdc.gov/coronavirus/mers/faq.html
http://www.bbc.com/news/health-28044151
Sunday, June 29, 2014
Sunday, June 22, 2014
Making Blood Culture Workups More Efficient
A major problem with blood culture workups is that it is often difficult to determine a true positive (pathogen) result from a false positive (contaminant) result. One solution is to adjust the testing algorithm in place. In 1970, it was shown that 11% of contaminated cultures had additional positive cultures, while 69% of clinically significant cultures had multiple positive cultures. In the proposed algorithm (summarized right), any
 isolates that are typically contaminants that are not present in follow-up cultures are reported as contaminants. To confirm the accuracy of the new algorithm, a nurse epidemiologist and an infectious diseases physician reviewed the patient charts.
isolates that are typically contaminants that are not present in follow-up cultures are reported as contaminants. To confirm the accuracy of the new algorithm, a nurse epidemiologist and an infectious diseases physician reviewed the patient charts.
Overall, organisms considered to be contaminants (CNS, diphthroids, Micrococcus spp, Bacillus spp, and viridans streptococci) were identified in 495/1040 positive blood cultures. Of the 495, 286 were classified as contaminants due to negative follow-up cultures, 171 were investigated by a pathology resident, and 15 were classified as pathogens (viridans strep with positive follow-up cultures). The majority (62%) of the contaminants were identified as CNS.
Two types of errors, VM (very major) and M (major) were used to determine the success of the new algorithm. A "very major error" occurred if an isolate that was classified as a contaminant was determined to be clinically significant after chart review. A "major" error occurred if an isolate was classified as indeterminate or pathogenic and was later determined to be not clinically significant. VM errors occurred in 6.3% of cases and M errors occurred in 6.6% of cases. Further adjustment of this algorithm may decrease the error rate in the future, but the algorithm was determined "acceptable" by the authors of this study.
Source: http://jcm.asm.org/content/40/7/2437.full
isolates that are typically contaminants that are not present in follow-up cultures are reported as contaminants. To confirm the accuracy of the new algorithm, a nurse epidemiologist and an infectious diseases physician reviewed the patient charts.Overall, organisms considered to be contaminants (CNS, diphthroids, Micrococcus spp, Bacillus spp, and viridans streptococci) were identified in 495/1040 positive blood cultures. Of the 495, 286 were classified as contaminants due to negative follow-up cultures, 171 were investigated by a pathology resident, and 15 were classified as pathogens (viridans strep with positive follow-up cultures). The majority (62%) of the contaminants were identified as CNS.
Two types of errors, VM (very major) and M (major) were used to determine the success of the new algorithm. A "very major error" occurred if an isolate that was classified as a contaminant was determined to be clinically significant after chart review. A "major" error occurred if an isolate was classified as indeterminate or pathogenic and was later determined to be not clinically significant. VM errors occurred in 6.3% of cases and M errors occurred in 6.6% of cases. Further adjustment of this algorithm may decrease the error rate in the future, but the algorithm was determined "acceptable" by the authors of this study.
Source: http://jcm.asm.org/content/40/7/2437.full
Friday, June 13, 2014
PED Virus Increasing Pork Prices
In May 2013, porcine epidemic diarrhea virus (PEDv) was isolated in hog herds in the United States. PEDv cause diarrhea and vomiting in pigs (morbidity near 100%) with variable mortality. Older pigs are more likely to survive the virus than young pigs (mortality 50-100%). The virus has an incubation period of 3-4 days, and is spread more slowly than other types of swine gastroenteritis. Pigs who recover do so within 7-10 days of symptom onset. The virus is spread through a fecal-oral route, but fomites and contaminated equipment may spread the virus as well.

PEDv was first reported in the United Kingdom in 1971, and has spread to several countries since then.
PEDv is a Coronavirus, containing an enveloped ssRNA genome. The virus does not appear to have jumped to humans in the 40 years since its discovery.
Global AgriTrends speculates that up to 4.5% of pigs, or 4.5 million hogs, in the US may be killed by PEDv this year. Some farms have lost 10% of their herds already. Pork prices are expected to increase 3% this year, compared to 0.9% last year. A vaccine is not yet available for the virus in the US, but there are vaccines currently available in South Korea, Japan, and China.
PEDv was first reported in the United Kingdom in 1971, and has spread to several countries since then.
PEDv is a Coronavirus, containing an enveloped ssRNA genome. The virus does not appear to have jumped to humans in the 40 years since its discovery.
Global AgriTrends speculates that up to 4.5% of pigs, or 4.5 million hogs, in the US may be killed by PEDv this year. Some farms have lost 10% of their herds already. Pork prices are expected to increase 3% this year, compared to 0.9% last year. A vaccine is not yet available for the virus in the US, but there are vaccines currently available in South Korea, Japan, and China.
Sunday, June 8, 2014
Bacteria Cultured from a Bear Bite
One of the dangers of an animal bite (aside from the trauma of the bite itself) is the possibility of infection due to flora in the mouth of the animal. If an infection does develop from an animal bite, knowing the flora present is helpful in choosing antibiotics that will be effective. Most animals that interact with humans (cats, dogs, etc) have well-defined flora. Less is known about other animals, such as bears, that rarely bite humans.
A case report from 2004 describes the bacteria cultured from a bite wound inflicted on a hunter by a grizzly bear in Canada. Cultures taken about 12 hours after the bite grew Serratia fonticola, Serratia
 marcescens (used to draw a raptor, right), Aeromonas hydrophila, Bacillus cereus, and Enterococcus durans. No anaerobes were isolated from the wound. The patient was given 1 week of piperacillin-tazobactam therapy followed by amoxicillin-clavulanate and ciprofloxacin for 3 weeks as prophylactic treatment.
marcescens (used to draw a raptor, right), Aeromonas hydrophila, Bacillus cereus, and Enterococcus durans. No anaerobes were isolated from the wound. The patient was given 1 week of piperacillin-tazobactam therapy followed by amoxicillin-clavulanate and ciprofloxacin for 3 weeks as prophylactic treatment.
Infection after a bear bite is common, with around 44% of patients showing infection. However, few of these bite wounds have been cultured for identification of flora, so there is limited knowledge of what is common or what antimicrobials are appropriate for treatment. Some scientists hypothesize that oral flora of bears will be similar to that of dogs, as well as being highly variable depending on the foraging environment and habits of a particular bear.
More information about the patient and his clinical outcomes can be found here: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC446265/#__ffn_sectitle
A case report from 2004 describes the bacteria cultured from a bite wound inflicted on a hunter by a grizzly bear in Canada. Cultures taken about 12 hours after the bite grew Serratia fonticola, Serratia

Infection after a bear bite is common, with around 44% of patients showing infection. However, few of these bite wounds have been cultured for identification of flora, so there is limited knowledge of what is common or what antimicrobials are appropriate for treatment. Some scientists hypothesize that oral flora of bears will be similar to that of dogs, as well as being highly variable depending on the foraging environment and habits of a particular bear.
More information about the patient and his clinical outcomes can be found here: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC446265/#__ffn_sectitle
Subscribe to:
Comments (Atom)